
by Kurchi Mitra
COVID-19 has left an indelible mark on nearly every country-sparing close to none in terms of the lives lost, the jobs impacted, the extended months of social isolation. However, countries in the Global South such as those in Africa, which experts feared would be ravaged by the pandemic due to their underfunded and overstretched public health systems, managed the pandemic, the numbers would suggest, better than many high income countries (HICs). Even accounting for the younger age demographic and other factors, there’s no denying that the African continent’s early implementation of lockdowns and strong adherence to core public health measures had a part to play in controlling the virus(1). Countries in the East and Asia Pacific, such as South Korea, which saw its first case within a day of the United States, experienced vastly fewer deaths than in the States (2). High-income countries of the Global North, such as the UK, European nations and the US, have been brought to their knees by a virus that other “less developed” countries seem to have coped with better. Even as we continue to learn the lessons from the pandemic and why some countries have fared better than others, this asymmetry has created a fertile ground to challenge the dominant paradigms of global health. The time is ripe to have a conversation about the lessons we have to learn from the Global South and the colonial attitudes about global health that persist to this day. In this piece, I will be discussing global health’s colonial roots and the effects it has on three key areas- power and funding, attitudes and research output, before going on to explore the meaning of “decolonising global health” and how we can go about doing so.
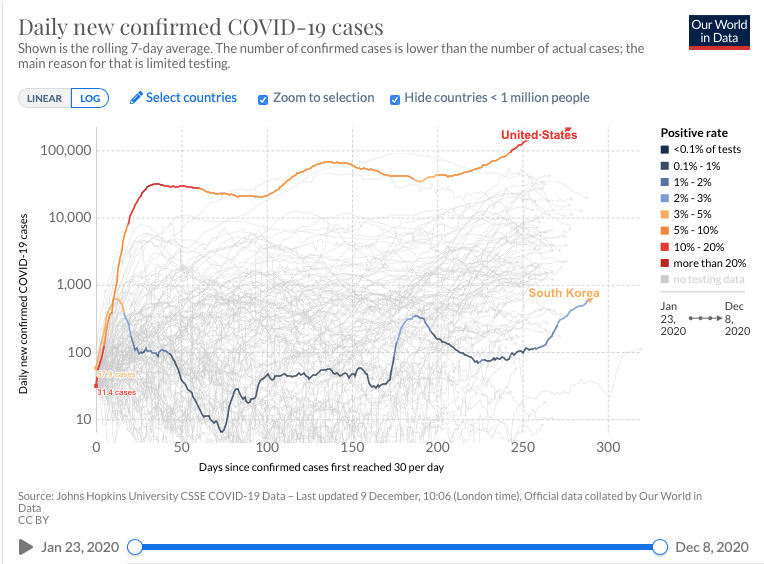
Source: Johns Hopkins University CSSE COVID-19 Data- Last updated December,10:06 (London time). Official data collated by Our World in Data
Global health and its colonial past
The history of the field of global health is marred by its colonial roots, which began with the intention of keeping tropical infectious disease safely locked up in the colonies, as a way to open up trade routes for profit and to “civilise” the masses.
Global Health’s colonial roots are not a thing of the past however. The origins of the London School of Hygiene and Tropical Medicine (LSHTM), a key player in research in former British colonies today, can easily be traced back to its colonial past. The most obvious link is the LSHTM founder, Patrick Manson, serving as the Chief Medical Officer to the Colonial Office(3), by the initiative of Joseph Chamberlain, then Secretary of State for the colonies to be better able to exploit the colonies’ resources(4). Following recent trends towards dismantling colonial era power structures, LSHTM and other colonial era institutions recognise their troublesome past and appear to be committed to understanding the consequences of their colonial histories, through research, funding and activism(3).
Health outcomes are intrinsically linked to wider social determinants such as social, economic, political, cultural, and ideological as well as external factors, which have no doubt been shaken by colonial history. The links between the stretched public health systems prevalent in many countries and their colonial past are intimately intertwined. The resources and governance of many countries were exploited under colonialism to facilitate extraction and dependence, not to set up well functioning public services, and these scars no doubt impact health systems to this day. Interestingly, the World Health Organization (WHO) faced significant backlash, from colonial powers, in establishing regional centres on the continent. This severely restricted the power of the WHO in establishing positive change in Africa, bound by the former colonialists who funded it (5).
- The Power Imbalance
There still remains major power asymmetries between the North and South in the global health sphere, rooted in economic power imbalances, lopsided global governance structures, racism and colonialism(6). The Global Health 50/50 report found that 85% of global organisations active in the healthcare field have headquarters in Europe and North America, with two-thirds in just three countries: Switzerland, UK and USA. Further, LMICs receive significant aid from global health organisations (UN, WHO) and philanthropists (Bill and Melinda Gates Foundation, Wellcome Trust) who, through their funding, hold the power to set health agendas. The report also found that more than 70% of leaders in a sample of 200 global health organizations are men, more than 80% are nationals of HICs and more than 90% were educated in HICs (6). This creates a global health architecture where powerful men, often older and white, sit in boardrooms in established colonial institutions in the Global North are responsible for setting the health agendas for countries miles away, with little to no significant involvement of local leaders.
2. Persisting Colonial Attitudes towards Global Health
Colonial attitudes of providing “aid” and “charity” to the ailing Global South still pervade. The “White Saviour complex”, wherein white people are seen as Messiahs, saving the underprivileged from their plight, underpins several brief “Voluntour” stints undertaken by gap-year students and many others to LMICs, in the name of philanthropy.
For medical students in particular, there have been questions raised about the practise of taking medical electives in low and middle income countries. A large number of students who choose to do their medical electives in LMICs-approximately 40% of British students and upto 59% of Australian students(7). The literature indicates several benefits to the visiting students, such as increased cultural exposure, assessing different career options etc. The benefits to the host countries are less clear, with few papers discussing its benefits and even going as far as to highlight detriments such as students being unfamiliar with prevalent health conditions, language barriers impacting patient communication, and the performance of medical procedures beyond the student’s experience (7).
Actors in the Global Health sphere must be cognisant of the fact that the Global South’s higher disease burden can be directly linked to the power imbalance created by colonialism. Hence, their working in the field should be seen as an act of humility, restoring what was taken, and not “The White Man’s Burden”.
The rapid unfolding of the COVID-19 crisis has merely shone the light on a fractured global health ecosystem, haunted by its colonial past. There was widespread uproar when two French scientists proposed using Africans essentially as guinea pigs, to test the effectiveness of the TB vaccine against COVID. World Health Organization Director Dr Tedros Adhanom Ghebreyesus went as far as to say “Africa cannot and will not be a testing ground for any vaccine. The hangover from colonial mentality has to stop. WHO will not allow this to happen.”(8)
3.Research imbalance
The colonial imbalances aren’t restricted to just funding and power. There is a noticeable skew towards the North in terms of research output, with scientific research trickling down from the North to the South (9) and troubling authorship trends, heavily skewed towards developed nations in Europe and North America (10). All but one Global health Journal is based in the West and a significant proportion of editors (upto 70%) are from HICs (11).This is highly problematic on a number of levels. The research may be entirely disconnected from the needs, infrastructure and facilities available on the ground, and the ones gaining from their implementation aren’t always the people they were designed to help. Diseases of relevance to high-income countries were investigated in clinical trials seven-to-eight-times more often than were diseases whose burden lies mainly in low-income and middle-income countries(12). Only 0.9% of international journal articles come out of the African continent, and 0.6% comes out of South Africa alone. This means that only 0.3% come from the 52 other countries on the continent, compared to North America and Europe producing 32% and 30% of the world research output(13).
COVID-19 has shown us that the Global South and East have valuable knowledge and experience in handling epidemics, which the North could potentially have benefitted from if there were a more bilateral exchange of research and ideas.
What do we mean by Decolonisation?
Decolonising global health has been cropping up recently in academic circles, student activism and the Twitter-sphere, but doesn’t have a set definition. My personal interpretation is that it would involve recognition of the colonial roots of global health and actively thinking of ways in which to dismantle them. The irony is not lost when we consider that the conversation about Decolonising Global Health is being had mainly in elite institutions of the Global North such as Harvard, Duke and Edinburgh, with a small number of non-western leaders, who themselves are educated in the Global North.


Renzo Guinto, a key player in the emerging field of Decolonisation, maintains that moving away from the traditional donor-recipient dynamic prevalent in global health and promoting diversity and inclusion amongst major Global Health institutions are important first steps(14). Global Health needs to start being global in the true sense of the word. Mutual learning, respect and bilateral distribution of knowledge and expertise.
It’s incredibly important to move beyond mere token gestures of Decolonisation. Adding a few people of colour on boards in colonial institutions doesn’t mean you’re decolonized.
It’s important for western leaders to move beyond the current paradigm, to invest in building capacity and empower leaders in the Global South to be able to set their own health agendas. One example of the above is the establishment of the University of Global Health Equity(15), that strives to work in close collaboration with local governments and communities to establish agendas regarding their own healthcare. Some concrete positive change has been made in this regard, beyond mere conversation. GAVI and the Global Fund have reconfigured representation on their boards and the Coalition for Epidemic Preparedness Innovations (CEPI) are shifting the global research agenda by prioritising vaccines that have traditionally been overlooked but disproportionately affect disadvantaged countries.(16)
It’s also crucial to involve actors from the Global South in this conversation. Having these conversations in elite, previously colonial institutions, be it a more representative group, still runs the risk of being utterly disconnected from the realities of healthcare halfway across the world and runs the risk of becoming the neo-colonisers, sending out decrees to people who have no on-the-ground experience.
Like all other areas in healthcare, constant reflection is important for actors working in this field to make sure they are doing more good than harm, despite their best intentions.
For more ideas!
- https://theconversation.com/global-health-still-mimics-colonial-ways-heres-how-to-break-the-pattern-121951
- https://www.un.org/development/desa/en/news/intergovernmental-coordination/south-south-cooperation-2019.html
- Can we re-imagine global health in a post-pandemic world?https://www.forbes.com/sites/madhukarpai/2020/04/06/can-we-reimagine-global-health-in-the-post-pandemic-world/?sh=70620ee84c22
- How Africa fought the pandemic — and what coronavirus has taught the world https://www.ft.com/content/c0badd91-a395-4644-a734-316e71d60bf7
- https://www.forbes.com/sites/madhukarpai/2019/11/10/global-health-research-needs-more-than-a-makeover/?sh=400c61707e34
References
- https://gh.bmj.com/content/5/10/e003319
- https://www.sciencedaily.com/releases/2020/08/200820102431.htm
- https://www.lshtm.ac.uk/sites/default/files/2020-01/chiph_colonialism_project_protocol.pdf
- Worboys, M. (1988). Disease, Medicine and Empire (R. MacLeod & L. Milton, Eds.). Retrieved from
- https://librarysearch.kent.ac.uk/client/en_GB/kent/search/detailnonmodal/ent:$002f$002fSD_ILS$002f0$002fSD_ILS:246910/one
- https://www.redpepper.org.uk/the-colonial-origins-of-africas-health-crisis/
- https://globalhealth5050.org/2020report/
- Crump JA, Sugarman J. Ethical considerations for short-term experiences by trainees in global health. JAMA. 2008;300(12):1456-1458. doi:10.1001/jama.300.12.1456
- https://www.devex.com/news/is-covid-19-magnifying-colonial-attitudes-in-global-health-97499
- Reidpath DD, Allotey P The problem of ‘trickle-down science’ from the Global North to the Global SouthBMJ Global Health 2019;4:e001719.
- Authorship trends in The Lancet Global Health
Iyer, Adithi R
The Lancet Global Health, Volume 6, Issue 2, e142 - Bhaumik S, Jagnoor JDiversity in the editorial boards of global health journalsBMJ Global Health 2019;4:e001909.
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)61046-6/fulltext
- Lillis, Theresa and Curry, Mary Jane (2010). Academic Writing in a Global Context: The politics and practices of publishing in English. Abingdon: Routledge.
- https://www.internationalhealthpolicies.org/blogs/decolonizeglobalhealth-rewriting-the-narrative-of-global-health/
- https://ughe.org
- https://www.forbes.com/sites/madhukarpai/2020/03/08/global-health-needs-to-be-global–diverse/?sh=4e8b2fd77659
- https://www.thinkglobalhealth.org/article/silenced-voices-global-health
